The Corporate Transparency Act (CTA) went into effect this year and requires businesses to disclose the identities and provide additional information about its beneficial owners, defined as or the individuals who ultimately control the company. Companies formed before January 1, 2024, must file their “beneficial ownership information” (BOI) reports to the Financial Crimes Enforcement Network (FinCen) no later than January 1, 2025. Companies created after January 1, 2024, must file their BOI reports within 90 days after receiving notice of formation or registration.1
This reporting requirement will apply to most professional medical corporations if they have fewer than 21 full-time employees or reported less than $5 million in gross receipts or sales in the previous year’s federal income tax returns.2 The company’s BOI report can be submitted to FinCen through a secure filing system available on its website: https://boiefiling.fincen.gov.
If you would like assistance with the filing requirement, please reach out to one of the listed attorneys.
Frequently Asked Questions
1. Which individuals are required to report their information?
Beneficial owners of reporting companies are the individuals who, directly or indirectly, either a) exercise substantial control or b) own or control not less than 25 percent of the ownership interests of the company.3
Individuals with substantial control over a reporting company include:
senior officers, such as the President, CFO, CEO, COO, or any other officer, regardless of official title, who performs a similar function;4
a person with authority over the appointment or removal of any senior officer or majority of the board of directors (or similar body); or
a person who can direct, determine, or have substantial influence over important decisions made by the company.5
The following individuals are not considered beneficial owners:
a minor child if the information of the parent or guardian is reported;
an individual acting as a nominee, intermediary, custodian, or agent on behalf of another individual;
an individual acting solely as an employee of the company and whose control over or economic benefits from such entity is derived solely from their employment status;
an individual whose only interest in the company is through a right of inheritance; or
Reporting companies created after January 1, 2024, must additionally report the company applicant, or the individual who filed the application to form the reporting company.7
2. What information is included in the initial BOI report?
The BOI report includes the beneficial owner’s:
full legal name;
date of birth;
current residential or business address;
the identification number from a valid US passport, driver’s license, government or Indian Tribe ID document, or foreign passport; and
If there is a change with respect to required information already submitted to FinCEN concerning the company or its beneficial owners’ information, an updated report should be filed within 30 calendar days after the date on which such change occurs.9
The BOI report also requests the following information about the reporting company:
full legal name;
any trade name or “doing business as” name;
complete current address;
the State, Tribal, or foreign jurisdiction of its formation or where it first registered; and
the Internal Revenue Service Taxpayer Identification Number.10
3. How often must BOI be reported?
BOI reporting is required only once, unless a company needs to update or correct information.11
4. Is BOI publicly available?
No, FinCEN will store the BOI in a secure nonpublic database. Additionally, BOI reports are exempt from disclosure under the Freedom of Information Act.12
Only certain government agencies may request access to BOI for security or tax activities. Otherwise, a financial institution, with the reporting company’s consent, may access the BOI to facilitate its compliance with customer due diligence requirements under applicable law.13
5. Are there penalties for noncompliance?
Yes, civil penalties will apply if a person fails to report or update BOI to FinCEN. Civil and criminal penalties will apply if a person willfully provides false or fraudulent information.14
6. Are spouses of beneficial owners required to comply with the reporting requirements?
Possibly. Current guidance suggests that if the business interest owned by an individual is characterized as community property under applicable law, both the named owner and the spouse would be considered beneficial owners, requiring both to be included in the CTA filing.15
7. Why is this information being collected?
The CTA was enacted in 2021 to aid law enforcement in combatting money laundering, tax fraud, terrorism financing, and other illicit activity conducted through anonymous shell companies. FinCen is a new bureau of the U.S. Department of Treasury.16
Executive Summary: This article provides an in-depth exploration of the nuanced interaction between Private Equity (PE) investments and medical group practices within the legal framework of California’s prohibition against the Corporate Practice of Medicine (CPOM). It critically analyzes the doctrine’s current application in California’s healthcare sector and its impact on the operational dynamics of medical practices post-PE acquisition. Moreover, the discussion extends to innovative structuring strategies that PE firms and healthcare practices can employ to align their operations with CPOM compliance while achieving their business objectives.
Understanding Private Equity Acquisitions and Recent Trends
In the past decade, there has been a remarkable surge in private equity (PE) firm involvement within the healthcare sector. PE firms have acquired a diverse range of healthcare facilities, effectively encompassing the entire spectrum of healthcare services. Independent physician medical practices have emerged as particularly attractive targets for these investments. PE acquisitions of physician practices rose from 75 deals in 2012 to 484 in 2021.1 This flood of PE healthcare acquisitions has contributed over $1 trillion in investments in the past decade.2
PE firms harness capital from high-net-worth individuals and institutions, often leveraging significant debt, to purchase companies. These firms typically aim for a rapid exit within three to five years and expect substantial profits.3 In fragmented markets, PE firms frequently adopt a strategy of making an “anchor investment” by initially acquiring a “platform practice,” which serves as a base for further acquisitions and consolidation within a specific region.4 A key characteristic of PE investments is their direct management involvement in the companies they acquire, frequently implementing changes to enhance valuation and future profitability prospects.5
The growing prevalence of PE ownership in healthcare has generated diverging opinions within the medical community. Critics argue that PE firms’ profit-centric approach compromises patient safety, saddles healthcare entities with excessive debt, and disrupts care through continuous management alterations and frequent sell-offs. In contrast, supporters of PE ownership highlight the injection of capital, managerial expertise, operational efficiency improvements, economies of scale, and the potential to align profit motives with the delivery of high-quality care. PE investments can also provide crucial capital and financial stability for medical groups seeking autonomy.
These converging opinions are further intensified by the distinctive nature of PE compared to other health services investments—the primary distinguishing factor being that PE firms are comprised of lay investors who are not bound by the same professional considerations as healthcare providers.6 Thus, the concern is that the PE investors’ interests conflict with healthcare providers’ duties to prioritize patient safety. This sentiment is consistent with the foundational principles of the prohibition on the corporate practice of medicine (CPOM), a legal principle enforced by several states, including California. The CPOM prohibition, sometimes called the corporate bar (on the practice of medicine), aims to prevent non-physicians from exerting undue influence over medical practices, thereby safeguarding the physician-patient relationship against commercial exploitation. As PE firms increasingly seek to acquire medical group practices, California’s CPOM prohibition acts as a critical checkpoint.
Legal Framework and Practical Considerations
California’s CPOM Doctrine
In the simplest terms, California’s CPOM doctrine prohibits non-physicians from owning or exercising control over medical practices. California’s corporate bar is designed to protect the clinical independence of physicians. It aims to ensure that medical decisions are made based on the patient’s best interests and not influenced by business considerations of non-physician owners or managers.
California’s CPOM prohibition is codified in two primary statutes:
Business and Professions Code section 2052 prohibits the unlicensed practice, attempted practice, or advertisement of practice of medicine in California, and makes these acts a misdemeanor. Importantly, the statute restricts medical practice to those who are duly licensed.
Business and Professions Code section 2400 explicitly prohibits corporations and other artificial legal entities from practicing medicine or employing physicians to provide professional medical services. This statute seeks to ensure that medical decisions are made by licensed medical professionals rather than corporate entities.
Key to carrying out California’s CPOM prohibition is the limitation on the corporate form available to medical practices. If medical practices want to incorporate, they must do so as professional medical corporations (PCs).7 With limited exceptions, licensed physicians must own and control these PCs.8 As such, a PE firm cannot purchase a medical practice outright.9
Friendly-PC Arrangements – the Typical Form
Despite California’s general prohibition, a corporate and contractual structure has been utilized to allow non-physicians to be involved in certain non-clinical aspects of a medical practice. This structure is often referred to as the “friendly-PC model,” and crucially, in return for providing non-clinical services, non-physicians are able to capture a portion of the medical group’s revenue.
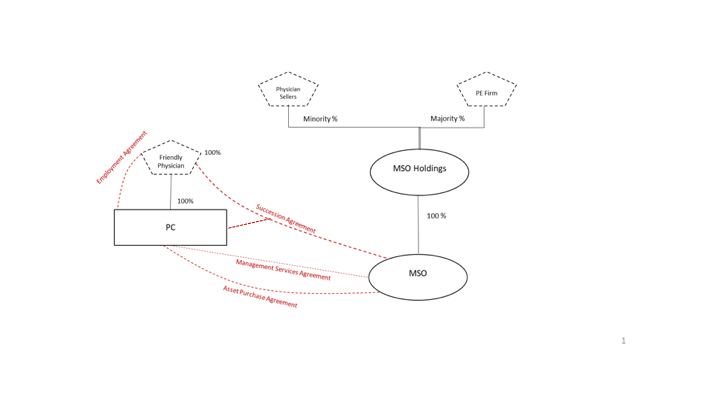
Under the friendly-PC model, the lay entity owns a management services organization (MSO) (sometimes called an administrative services organization), which contracts with a PC through a management services agreement. The PC is solely owned and governed by a licensed physician who is “friendly” to the MSO.
The management services agreement entrusts the MSO with exclusive oversight of the administrative and managerial aspects of the PC in exchange for a management fee paid by the PC to the MSO. In this arrangement, the MSO manages all non-clinical and operational facets, including owning leases and equipment and employing non-clinical staff. The MSO collects a management fee from the PC, which could be a flat monthly fee, based on a percentage of the PC’s revenues, or a combination of the two. Importantly, however, the management fee must be commensurate with the MSO’s services, equipment, or facilities rendered and cannot equate to a sharing of the practice’s profits.10
This connection between the PC and MSO is often reinforced through a succession agreement. A succession agreement allows the MSO to appoint a new shareholder to the PC in response to specific events, such as an attempt by the physician to terminate the management services agreement. Often, the MSO can freely eject the friendly physician without cause. Because the MSO essentially has the power to eject the friendly physician via the succession agreement, the MSO maintains a certain level of control over the PC’s operations.
Friendly-PC Arrangement in the Context of a PE Acquisition
In the PE context, the PE firm will first form (or cause the PC to form) the MSO. Next, the friendly physician will cause the PC to transfer and assign its non-clinical assets to the MSO, including, where appropriate, the PC’s goodwill. In exchange for the PC’s non-clinical assets, the MSO will pay the PC a considerable amount of cash and issue rollover equity in the MSO or the MSO’s parent entity. The purchase price is financed through debt secured against the acquired entity itself.11 Some PE firms secure loans using their healthcare facilities as collateral, repaying investors quickly while the facilities assume the debt. They also sell healthcare assets to other investors, using the proceeds for returns and then leasing the assets back to the healthcare organizations.12
Simultaneously, or soon thereafter, the PC will be reorganized so that it is solely owned and operated by the friendly physician. If the PC has more than one shareholder, the PC will cause the redemption of all shareholders other than the friendly physician. The MSO, PC, and friendly physician then enter into the management services and succession agreements, as applicable.
Finally, the parties’ purchase agreement often requires the PC to deliver executed professional services agreements (i.e., independent contractor or employment agreements) for each of its contracted providers before closing. The MSO wants to ensure that the PC’s providers will continue treating their patients as they did immediately before closing.
The diagram below illustrates a simplified version of the relationships between the various entities post-close.
Other considerations in these deals concern the ownership and control of the MSO and, more specifically, how the MSO’s profits are eventually distributed to the MSO’s owners. Post-close, the PE firm holds a majority stake in the MSO (or its parent), while the physician sellers collectively own a minority stake. The owners’ rights (and ability to control the MSO) will depend on the approval rights allocated to minority interest holders under the governance documents of the MSO or its holding company.13
PE Healthcare Acquisition Impacts and Legal Responses
Impact of PE Acquisitions on Quality, Cost, and Accessibility of Healthcare
The impact of PE healthcare acquisitions is the subject of ongoing debate. PE backers and supporters alike have documented important benefits to PE healthcare acquisitions, including:
Funding innovation and streamlining costs, especially in critical areas like telehealth and healthcare IT.14
Supporting clinical trials and unlocking lifesaving treatments like mRNA vaccinations15.
Helping consolidate medical groups’ market power and obtain favorable reimbursement rates16.
Offering healthcare providers a source of capital and relieving them of management responsibilities.17
Significant upfront cash payments that are much more than traditional asset purchase transactions proposed by other health systems.18
Critics often raise concerns about the prioritization of profit over patient care, potential reductions in the range of services offered to maximize profitability, and the long-term sustainability of such investments. Studies have found that this profit-centric approach has led to:
An average increase of $71 (+20.2%) in charges per claim following PE acquisition.19
An increase of $23 (+11.0%) in the allowed amount per claim.20
An increase in overutilization of services and increased spending without commensurate patient benefits, raising important considerations for policymakers.21
A higher clinician replacement ratio compared to non-PE-acquired practices.22
Statistically significant per-patient expenditure increases for private physician practices.23
An increase in patient falls, infection, and other forms of harm during hospital stay after a PE acquisition.24
In sum, while there are operational efficiencies, the focus on profit margins can sometimes lead to cost-cutting measures that can negatively affect patient care and employee satisfaction.
Legal and Regulatory Responses to PE Healthcare Acquisitions
California’s government bodies have been paying closer attention to the increasing trend of PE investments in healthcare, responding with heightened scrutiny and regulatory measures.
In 2020, the California Legislature considered Senate Bill 977,25 which aimed to grant the California Attorney General greater oversight power over healthcare transactions, including those involving PE firms. It sought to require the AG’s office to review and approve acquisitions of healthcare facilities by large health systems and private equity groups, particularly focusing on transactions that might reduce competition and increase healthcare costs. SB 977 did not pass, though a similar bill has been introduced in the current legislative session.26
In 2023, Senate Bill 184 established the Office of Health Care Affordability (“OHCA”) within the Department of Health Care Access and Information.27 OHCA adopted regulations on December 18, 2023,28 to implement the cost and market impact reviews established by Health and Safety Code section 127507 et seq. The laws obligate specific “health care entities”29 to notify OHCA about a “material change transaction”30 that could affect market competition or healthcare costs. OHCA has 60 days post-notification to decide whether to conduct a more intensive cost and market impact review of the transaction.31 If OHCA decides to conduct the review, the process may take up to eight months,32 potentially causing lengthy delays in closing. Reviews focus on market effects, service pricing, and quality, among other factors.33 Preliminary and final reports are issued, with a mandatory waiting period before transaction completion.34
OHCA’s oversight of material change transactions will likely lead to increased scrutiny of qualifying PE healthcare acquisitions. The new law’s pre-transaction notice requirements and regulatory review may deter PE firms from investing in California healthcare entities. At the very least, we anticipate that PE firms will be more cautious and selective in their California healthcare acquisitions.
Laws that may impact PE acquisition of medical practices are also developing through litigation. For example, in 2020, Allstate Insurance Company filed two complaints alleging that several radiology practices managed by Sattar Mir, who has no medical license, submitted fraudulent insurance claims.35 Among other issues, the parties disputed whether Mir’s control over medical corporations through an MSO constituted the unlicensed practice of medicine.
In its complaints, Allstate alleged that Mir illegally practiced medicine by forming and owning medical corporations, soliciting patients, selecting physicians to perform radiology services, and making decisions regarding billing and collections. After suffering dismissals in the Los Angeles County Superior Court, Allstate prevailed on appeal in August 2023. The appellate court ruled that Allstate had sufficiently alleged that Mir engaged in the unlicensed practice of medicine by exercising undue control over the radiology practices, and Allstate may, therefore, bring claims under the Insurance Fraud Prevention Act and Unfair Competition Law (UCL).36 The California Supreme Court denied the defendants’ petition for review, allowing Allstate to proceed with its lawsuits.
Challenges to the friendly-PC model have also emerged in federal court. In 2021, the American Academy of Emergency Medicine Physician Group (AAEM) sued Envision Healthcare under the UCL for allegedly using restrictive management contracts to control hundreds of medical practices.37 AAEM claimed that Envision exercised discretion over physicians’ hiring, compensation, schedules, billing, contracts with third-party payors, and ability to sell their practices. Further, Envision allegedly established clinical oversight over the physicians by establishing corporate standards of care. The Northern District of California denied Envision’s motion to dismiss the lawsuit, ruling that AAEM had sufficiently alleged that Envision violated the ban on the corporate practice of medicine.38 However, the case has been stayed because Envision filed for Chapter 11 bankruptcy.
These recent legal developments are indicative of enhanced scrutiny of healthcare mergers and acquisitions, especially those involving PE firms. We anticipate that California’s laws governing PE investments in healthcare may become more stringent, creating increased oversight and regulation of such transactions.
Practical Considerations
Balancing Control Over the PC Post-Close
PE firms are incentivized to maintain as much control over the healthcare practice as possible. A PE firm will try to delegate to itself the most decision-making authority possible in the management services agreement. If the decision does not implicate professional medical judgment, the PE firm can contract for total control. Examples include: (1) management and administration of the non-medical aspects of the practice; (2) employment, management, hiring, training, supervising, and firing of the non-clinical personnel; (3) providing and maintaining the premises where the practice operates; (4) purchasing supplies for the practice; (5) bookkeeping and accounting services; and (6) billing and collecting on behalf of the practice.
For those decisions that could implicate professional medical judgment, the PE firm will still try to obtain decision-making authority so long as the physician is ultimately responsible for the decision. In practice, the management services agreement will often require that the MSO be consulted for all decisions regarding: (1) control of patients’ medical records, including determining what is or is not recorded therein; (2) selection, hiring, or firing of physicians, allied health staff, and medical assistants for reasons related to clinical competency; (3) setting the parameters under which the physician will enter into contractual relationships with third-party payers; (4) decisions regarding coding and billing procedures for patient care services; and (5) approving of the selection of medical equipment and medical supplies for the medical practice.
Ensure the Management Fee Bears a Reasonable Relationship to the Services Provided.
To safeguard against the appearance of undue control by the MSO, the management fee should bear a reasonable relationship to the MSO services. This is especially important when part of the management fee is for marketing services (e.g., when the MSO markets the medical services to referral sources such as patients).39 The management fee may be structured using one or a combination of three systems:
Percentage of Practice Revenue: This fee system helps align the financial incentives of the MSO with those of the PC and is relatively simple to calculate.40 This is perhaps the most common fee system.
Fixed Fee: This fee is generally permitted but represents a challenge as accurate budgeting is difficult.
MSO’s Costs Plus Markup: This fee is also generally permitted but may be difficult to administer and may not align the MSO’s financial incentives with those of the PC.
Provider Pitfalls
Indemnity: For smaller-scale physician practices, the selling physician-owners are often named as parties to the purchase agreement. As a named party, the selling physicians make (in their individual capacity) representations and warranties regarding the practice’s viability and compliance. If the buyer incurred any damages or costs resulting from a breach of these representations and warranties, the selling-physician owners may be obligated to indemnify the buyer for the company’s pre-closing conduct. In practice, personal liability is often not disclosed or discussed during the initial negotiations, and so it can come as a surprise for physician sellers. It is important that physician sellers understand any personal indemnity obligations, and if uncomfortable with the associated risk, limit or remove them.
Adverse Events: The MSO’s (or its parent entity’s) Operating Agreement will identify the events that trigger the redemption of the selling physicians’ ownership interests. Depending on the triggering event, the redemption price is usually the fair market value of the interests (a “Non-Adverse Event”) or a far lesser amount (an “Adverse Event”). In our experience, the MSO’s Operating Agreement will define an Adverse Event as broadly as possible to justify its redemption of the physicians’ interests for a low price. Common Adverse Events include (1) the termination of the physician’s relationship with the PC or MSO for cause, (2) the physician’s breach of his/her employment agreement, the Operating Agreement, Purchase Agreement, or affiliated transaction document, (3) the termination of the physician’s relationship with the PC or MSO (for whatever reason) before a certain time (more on this below), and (4) the physician’s voluntary withdrawal from the PC or MSO. In the last instance, if the physician decides to end his employment, the MSO could repurchase the physician’s interest in the MSO for an adverse price—sometimes as low as one dollar. While the physician’s negotiating power is rather limited, you can protect the physician’s equity by limiting the definition of an “Adverse Event” to cover only egregious conduct.
Employment Term and Non–Compete: Sometimes, the PE firm will entice the selling physician to sign an employment agreement with a mutual without-cause termination provision. At first glance, the physician can seemingly terminate his or her employment at any time with advanced notice. However, the physician is usually promised equity in the MSO, and as such, consents to the MSO’s Operating Agreement. As mentioned above, an Adverse Event can include the physician terminating his or her relationship with the PC or MSO—for whatever reason—within a specified period (such as one or more years) from the closing date. Thus, while the physician has the right to leave the PC for any reason under his or her employment agreement, the Operating Agreement inevitably deters the physician from leaving the PC for several years. Moreover, the Operating Agreement almost always restricts the physician’s ability to practice medicine in a specified territory even after this “probationary period” has lapsed. It is in the physicians’ best interests to reduce the “probationary period” and again limit the Operating Agreement’s definition of Adverse Event to allow a physician to terminate his or her employment without cause and without consequence.
Conclusion
Given the complexity of California’s CPOM prohibition, the impacts and outcomes of PE healthcare acquisitions in the State are inevitably nuanced. As California continues to scrutinize and potentially tighten regulations around healthcare acquisitions, PE firms must adapt, and the heavily relied upon friendly-PC workaround may be forced to evolve. The fluctuating regulatory environment may lead to more cautious investment approaches or creative structuring of deals to align with legal requirements.
Alexander Borsa, Geronimo Bejarano, et al., Evaluating trends in private equity ownership and impacts on health outcomes, costs, and quality: systematic review, The BMJ (July 19, 2023), https://www.bmj.com/content/382/bmj-2023-075244. ↩︎
Cal. Corp. Code §§ 13400-13410. Accordingly, medical practices cannot incorporate as LLCs, non-professional corporations, or limited partnerships. § 13405; Cal. Bus. & Prof. Code § 2400 et seq. Medical groups can be structured as a general partnership or operate without any corporate form (often referred to as “sole proprietorships”). Cal Bus. & Prof. Code § 2285. ↩︎
Under the Moscone-Knox Professional Corporation Act, physicians are allowed to incorporate as professional medical corporations, provided the corporations are owned and governed by licensed physicians. Cal. Corp. Code §§ 13406-13407; Cal. Bus. & Prof. Code § 2406. Certain non-physician employees, like registered nurses or physician assistants, are permitted under specific conditions. Cal. Corp. Code § 13401.5; Cal. Bus. & Prof. Code § 2408. ↩︎
Both stock and asset sales are effectively embraced by the requirement that medical groups incorporate as PC. For example, a lay entity cannot purchase the stock of a PC because lay entities cannot own the stock of a California PC. Similarly, a PE firm could not employ the medical group’s physicians for the purpose of treating patients. ↩︎
See Epic Med. Mgmt., LLC v. Paquette, 244 Cal. App. 4th 504, 516 (2015) (clarifying Bus. & Prof. Code § 650(b) permits contracts between physicians and non-physicians basing compensation on percentage of gross revenue if fee is commensurate with the MSO’s services being provided). ↩︎
PE firms often prefer to create a holdings company that will own 100% of the MSO’s interests. Owning an indirect interest in the MSO via a holdings company, as opposed to owning an interest in the MSO directly, can better facilitate the transfer of ownership or the sale of the healthcare practice and its associated assets. Moreover, separating the MSO from the PE firm’s main operations shields the PE firm from potential liabilities arising from the healthcare practice or the MSO’s operations. This structure can also provide tax advantages by allowing for more flexible structuring of the ownership and distribution of profits. ↩︎
A material change transaction occurs if a healthcare entity meets one of the eight thresholds enumerated under 22 C.C.R. § 97435(c), such as a transaction that results in transfer of control or governance, a transfer of a significant portion of assets, or a likely increase in annual revenue of $10 million or 20%. ↩︎
People ex rel. Allstate Ins. Co. v. Discovery Radiology Physicians, P.C. (Super. Ct. Los Angeles County, Nov. 5, 2020, 20STCV42672); People ex rel. Allstate Ins. Co. v. OneSource Medical Diagnostics, LLC (Super. Ct. Los Angeles County, Nov. 24, 2020, 20STCV45151). ↩︎
People ex rel. Allstate Ins. Co. v. Discovery Radiology Physicians, P.C. (2023) 94 Cal.App.5th 521, review denied (Nov. 21, 2023). ↩︎
American Academy of Emergency Medicine Physician Group, Inc. v. Envision Healthcare Corporation (N.D. Cal., Dec. 20, 2021, No. 22-CV-00421-CRB). ↩︎
See Epic Medical Management, LLC v. Paquette, 244 Cal. App. 4th 504 (2015) (court rejected physician’s argument that some management fee payments to MSO constituted illegal kickbacks for MSO’s marketing services in which some patients were referred to physician through marketing activities, finding no illegal payment for referrals occurred because management fee was commensurate with services rendered). ↩︎
Unlike some other states, California does not consider this fee system to violate anti-kickback law so long as the fee “is commensurate with the value of the services furnished[.]” Cal. Bus. & Prof. Code § 650(b). ↩︎
Governor Newsom signed California Senate Bill 1120 (SB 1120) in September 2024, introducing significant reforms to how health plans and disability insurers use artificial intelligence (“AI”) in utilization review (“UR”) decisions. This new legislation modifies Section 1367.01 of California’s Knox-Keene Health Care Service Plan Act of 1975 (pertaining to health care service plans) and Insurance Code § 10123.135 (pertaining to disability insurers).
UR and utilization management (“UM”) refer to the processes used by health plans and insurers to determine the medical necessity of a healthcare service, treatment, or equipment. Existing California law mandates health care service plans and disability insurers to implement UR policies governing the approvals, modifications, delays, or denials of health care services before, after, or at the time services are rendered. SB 1120 expands the scope of California’s current laws to include the use of AI by health care service plans, disability insurers, and their contractors in UR or UM related decisions.
Key Components of SB 1120
The bill mandates that health care service plans, disability insurers, including specialized plans, and such entities’ third-party contractors, that use AI or other AI-based tools for UR/UM medical necessity decisions comply with the following:
Criteria for AI-Based Determinations: AI systems must make decisions based on a combination of the enrollee’s medical history, individual clinical circumstances, and other relevant medical records. The legislation prohibits decisions based solely on group datasets.
Non-Displacement of Human Judgment: Entities subject to SB 1120 cannot use AI to replace the decision-making role of licensed physicians or other healthcare professionals. While AI can support the review process, final determinations about medical necessity must be made by licensed physicians or healthcare professionals who are “competent to evaluate the specific clinical issues involved in the health care services requested by the provider.”
Transparency and Compliance: The law requires health care service plans and disability insurers to maintain clear policies and procedures that establish how the plans or insurers review, approve, or deny providers’ requests for health care services based on medical necessity. This requirement includes making AI processes available for audits and compliance reviews, as well as ensuring that plans and insurers use patient data in accordance with privacy laws like HIPAA. Entities covered under the new law must also disclose the use of AI tools to their patients and providers upon request.
Prohibition of Discrimination: AI platforms and tools must be applied “fairly and equitably.” The legislation does not provide detailed guidance on the criteria for the fair and equitable application of AI, which creates challenges for compliance and may lead to disputes. Additionally, the bill explicitly requires that AI-based reviews must neither directly nor indirectly discriminate against any enrollee. Compliance with state and federal anti-discrimination laws is crucial for health plans using AI.
Periodic Review and Adjustment: Health care service plans, disability insurers, and their respective contractors performing UR/UM functions must regularly evaluate and update the performance of AI systems to ensure accuracy and effectiveness in decision-making processes.
Entities and Conduct Subject to SB 1120
SB 1120’s requirements apply not only to health care service plans regulated under the Knox-Keene Health Care Service Plan Act and disability insurers regulated by California’s Department of Insurance that cover hospital, medical, or surgical expenses, but also to third-party contractors that deploy AI technologies to assist with UR and UM functions. For example, if a health plan contracts with an AI company to assist in these UR/UM functions, the AI tools used by the company must comply SB 1120’s requirements, including its fairness, equity, and non-discrimination stipulations.
For the purposes of SB 1120, “AI” means “an engineered or machine-based system that varies in its level of autonomy and that can, for explicit or implicit objectives, infer from the input it receives how to generate outputs that can influence physical or virtual environments.” Willful violations of the new law constitute a crime.
Practical Impacts on UR/UM with AI
The law’s requirements for enhanced regulatory oversight are likely to increase administrative burdens on covered health plans, insurers, and their contractors that provide AI services, as they must ensure compliance through detailed documentation and disclosures. To the extent health plans are contracting UR/UM functions to AI-using vendors, the parties will need to navigate how compliance responsibility will be contractually allocated, and the vagaries of the law (e.g., ensuring AI is used “fairly and equitably”) may make this challenging.
Additionally, SB 1120 entrenches human decision-making as mandatory for UR, and firmly positions AI as a decision-support tool rather than a decision-maker. By mandating that licensed healthcare professionals make final determinations about medical necessity, health care service plans and disability, insurers cannot supplant human clinical judgment with technology.
Finally, SB 1120 seeks to make the decision-making process more transparent and understandable for patients. This aspect of the bill may enhance patient trust in AI-assisted healthcare, permitting them to gain clearer insights into how decisions are made. On the other hand, patients’ ability to request human review could increase the number of cases where AI recommendations are re-examined.
Health care service plans have increasingly used Artificial Intelligence (“AI”) to automate prior authorizations, process claims, and manage health outcomes, arguing it reduces costs and increases consistency. However, concerns about AI errors, biases, and unwarranted coverage denials have caused California and other states to curb AI’s uses to prevent discrimination and protect patient rights.
Of particular interest is California’s SB 1120 (“The Physicians Make Decisions Act”), which has already passed in the State’s Senate and is advancing quickly through the Assembly. SB 1120 is designed to regulate the use of AI and algorithms in health plans’ prior authorization decisions and management functions by ensuring that AI-based determinations are made with adequate human oversight.
Insurers and health plans use prior authorizations as a tool to determine whether a health care service or treatment is medically necessary. While health plans and insurers are subject to certain regulatory requirements in California, existing law does not expressly limit these entities’ use or application of AI when making patient coverage determinations. SB 1120 would require denials, delays, or modifications of health care services based on medical necessity be made by a licensed physician or other competent health care provider.
The bill further mandates that AI tools used for prior authorization base decisions on an enrollee’s medical history and individual clinical factors. Finally, the use of AI tools must not directly or indirectly discriminate against individuals based on race, gender, age, disability, or other protected characteristics, be open to inspection, and comply with existing medical privacy laws.
Since 2015, the California Labor Code requires all employers to provide their employees with a minimum number of paid sick days. This requirement applies regardless of whether the employer establishes a paid sick leave policy or a paid time off (“PTO”) policy. Effective January 1, 2024, Senate Bill 616 amended the Labor Code by, among other things, increasing the required minimum amount of annual paid sick leave from 24 hours or three days to 40 hours or five days.
The complexity of this legislation can make it challenging for employers to ensure that their sick leave or PTO policies are legally compliant. To provide guidance, below is a summary of what we believe most California employers need to understand and integrate into their 2024 employment policies going forward.
First, a brief overview of the law- California employees’ right to paid sick leave is established under the Healthy Workplaces, Healthy Families Act of 2014 (the “Act”).1 The Act states that an employee who works for the same employer for at least 30 days within a year is entitled to a minimum amount of paid sick leave. SB 616 expands the Act by amending Sections 245.5, 246, and 246.5 of the California Labor Code and increases the required amount of annual paid sick leave from 24 hours or three days to 40 hours or five days.
Employers are required to provide paid sick leave upon an employee’s oral or written request for the following purposes:
diagnosis, care, or treatment of an existing health condition of, or preventive care for, an employee or an employee’s family member; or
time for an employee who is a victim of domestic violence, sexual assault, or stalking, to obtain relief to help ensure their or their child’s health and safety from crime or abuse.2
One of the most important aspects of this legislation is the extremely broad definition of who qualifies as suffering from the health condition that justifies paid sick leave. The law states that it applies to an employee or an employee’s“family member.” Family members include an employee’s spouse, registered domestic partner, child of any age (whether adopted, foster, or biological), parent, stepparent, foster parent, and legal guardian of either the employee or of the employee’s spouse. It also applies to a grandparent and to any sibling of the employee. Finally, it applies to whom the law refers to as a “designated person.” Employees are entitled to designate one person in any 12-month period to become a family member. There is no requirement that the designated person be living with the employee, and there is no requirement that the designated person be ill or injured since the definition of family member applies for the “preventative” care of designated persons as well.3
When establishing a paid sick leave policy, an employer is free to adopt one of two approaches: accrual or frontload. Each approach has unique aspects which are summarized below.
Accrual Approach
Under an accrual approach, employees earn (or accrue) paid sick leave throughout the year. The employee has the choice of three accrual approaches:
The employer may provide the employee with one hour of sick time for every 30 hours worked, beginning either at the commencement of employment or January 1, 2024, whichever is later, subject to the accrual limits provided in the legislation; or
The employer may use any alternative method of accrual, as long as sick leave time is accumulated “on a regular basis” and as long as the employee will have accrued at least 24 hours of accrued sick leave by the 120th day and 40 hours by the 200th day, measured from (a) the beginning of the calendar year, (b) the beginning of the employee’s employment, or (c) any other 12-month period the employer selects and applies; or
If the employer elects to have the 12-month period begin on the employee’s first day of employment, the employer may elect for the employees to accrue “days” as an alternative to accruing “hours.” If a day-accrual approach is used, then the employee must have accumulated at least three days by the completion of the 120th day of employment and five days by the 200th day of employment.4
When might it be advantageous for an employer to use the “day” accrual method (see (3) above) as opposed to the “hours” accrual method? If the employee works less than an 8-hour day, then the day accrual method would appear to make more sense. Otherwise, the part-time employee will reap a windfall from the wording of the legislation.
Example: Assume the employee is part-time, working 6-hour days. The employer’s policy permits all employees, part-time and full-time, to accumulate one hour of leave for every 30 hours worked. At that rate, in every five days of employment (or in one week’s time), the 6-hour employee will have accumulated one hour of sick leave. By the 40th week, the employee will have accrued 40 hours of leave (The maximum required by law if the hours’ method is used.). Since the employee only works 6 hours a day, 40 hours of sick leave will provide that employee with the equivalent of 6.6 days off each year. Instead, if the employer used the day accrual method, the employee’s sick days can be capped at 5 workdays (or 30 hours of paid sick leave each year).
As pointed out above, the law requires that the employer permit the employee 40 hours or five days of paid sick leave in a 12-month period; however, if the employer does not wish for the employee to be entitled to more sick days than the minimum mandated by the legislation, it is important that the employer’s policy impose a cap that is consistent with this legislation.
Example: Assume the accrual rate is one hour per 30 hours worked (see (1) above), and the employee works 8-hour days. In that case, the employee will likely accrue more than 40 hours by year’s end.
Example: Beginning on January 1, 2024, the employee works 8 hours per day, five days per week, throughout the year and takes three weeks’ vacation, leaving 49 weeks in which the employee works. Without a cap, the employee will accrue about 65 hours of sick time by the end of the year.
Further, if an employer uses the accrual approach, then employees are entitled to carry over unused, accrued sick leave from year to year. We will refer to those carried over sick days as being applied to a “subsequent year.” The employer may impose up to two additional caps: one cap on the number of paid sick days in any single subsequent year and a second cap on the total number of accrued sick days for all subsequent years. For those sick days the employee may take in any single subsequent year, the employer may, if it chooses, impose a cap of 40 hours or 5 days, and this cap may (but is not required to) limit both to the carried over days and the currently accruing days in the subsequent year to 40 hours or 5 days. Finally, the employer may impose a cap on the total number of days that are accruable for all subsequent years to 80 hours or ten days.5
Frontload Approach
Under the frontload approach, employers again have the choice of “hours” or “days.” Employers using this approach provide employees with either the full 40 hours or full five days of paid sick leave upfront at the beginning of a 12-month period. If an employer establishes a frontload policy, employees are not entitled to carry over unused sick leave from one year to the next. Employers are free to use either the employee’s first day of employment, the calendar year, or any other 12-month period as the time frame for compliance.6
Under either an accrual policy or a frontload policy, the employer may limit a new employee’s use of paid sick leave until the employee’s 90th day of employment. Employers may also set a minimum of two-hour increments for each time paid sick leave is used, but they cannot require their employees to take an entire day of paid sick leave off at a time.
Frequently Asked Questions
Can employees borrow unaccrued time for paid sick leave?
Yes, employers have the discretion to lend paid sick leave before it is accrued. They may also allow new employee to use paid sick leave before meeting the 90-day employment requirement.
Do California’s paid sick leave laws apply to exempt and nonexempt employees?
Yes, this legislation applies both to exempt and nonexempt employees. The main difference between exempt and nonexempt employees is that the California Department of Industrial Relations’ wage and overtime laws apply to nonexempt employees, but they do not apply to exempt employees.
Can employers request medical certification when an employee uses paid sick leave?
We do not recommend requesting certification when an employee uses paid sick leave. Employees are entitled to take paid sick leave immediately upon oral or written request, assuming they confirm that it is for their or a “family member’s” care, and employers may not deny paid sick leave solely based on a lack of certification. The law does permit, in theory, employers to reasonably request certification before payment for sick leave if they have information indicating that the employee is not requesting leave for a valid purpose. However, facts falling into this exception would be unusual. In effect, this law provides employees with up to five paid workdays off per year with little or no medical confirmation.
Are employers required to notify employees of their right to paid sick leave?
Yes, employers must display a poster notifying employees of their paid sick leave rights in a format that can be easily read at a location that is frequented by employees during the day.
The posting at the workplace should state the following:
An employee is entitled to accrue, request, and use paid sick days.
The amount of paid sick days provided for under Article 1.5 of the California Labor Code.
The terms of use of paid sick days.
That retaliation or discrimination against an employee who requests or uses paid sick days is prohibited and that an employee has the right to file a complaint with the Labor Commissioner against an employer who retaliates or discriminates against the employee.7
How does this legislation apply to employers with a PTO policy?
Under a PTO policy, employers do not distinguish between time off for reasons related to illness or injury and time off for other personal reasons, including vacations. Employers who have PTO policies are required to assure that the terms and conditions of this Act, in all respects, apply to employees who wish to take a PTO day off. In other words, the employer’s PTO policy must, at a minimum, satisfy all of the conditions and terms placed upon the sick leave requirements under this Act.
Effective January 1, 2024, Senate Bill 848 amended the California Fair Employment and Housing Act. This amendment established that California employees now have a right to “reproductive loss leave.” Reproductive loss leave entitles employees to take time off from work if they endure what the law calls a “reproductive loss event.” A reproductive loss event is defined as a failed adoption, a failed surrogacy, a miscarriage, a stillbirth, or an unsuccessful assisted reproduction.
This latest reason for taking leave from work applies to all employers with five or more employees. The employee can take up to five days’ leave, and the days do not have to be consecutive. Reproductive loss leave must generally be taken within three months of the reproductive loss event.
Frequently Asked Questions
Does this leave only apply if the employee personally suffers a reproductive loss event?
No, all of the recognized events which trigger this right to a leave (a failed adoption, failed surrogacy, stillbirth, unsuccessful assisted reproduction, and miscarriage) apply to both persons who would have been parents if the reproductive loss event had not occurred.
Are employers required to pay employees while they are on reproductive loss leave?
No, reproductive loss leave is unpaid, but employees may use any compensatory time off that is otherwise available to them such as vacation, personal leave, or sick leave.
How soon after a reproductive loss event must employees take reproductive loss leave?
Generally, reproductive loss leave should be completed within three months of the reproductive loss event. Employees are entitled to take leave on nonconsecutive days.
Can employers request medical or legal verification before employees take leave?
It is important that the employer not prevent the employee from taking this leave by requiring any kind of advance confirmation or verification. The legislation expressly states that the employee is entitled to exercise reproductive loss leave without the “employer’s interference or restraint.” However, it is always appropriate for the employer to request medical or other appropriate confirmation after the employee has taken all or part of the leave, and, if the employee cannot provide reasonable confirmation that a reproductive loss event has occurred, the employer should be able to take disciplinary action.
Are employers required to notify employees of reproductive loss leave?
No, the law does not require employers to notify their employees of reproductive loss leave.
Reproductive loss leave needs to be viewed as the latest in an increasing list of mandated leaves in California. Briefly, the other mandated leaves are as follows:
The California Family Rights Act (CFRA) entitles employees to take unpaid, job-protected leave for up to 12 workweeks during a 12-month period for the following reasons:
The birth, adoption, or foster placement of a child.
Taking care of a spouse, child, parent, or other designated person with a serious health condition.
The employee’s own serious health condition.
CFRA applies to all employers with five or more employees. Employees are eligible for CFRA leave after working for the same employer for more than 12 months and at least 1250 hours.1
California’s Pregnancy Disability Leave (PDL) entitles employees to take unpaid, job-protected leave for up to four months per pregnancy for any disability related to the pregnancy, childbirth, or related medical condition. This applies to all employers with five or more employees. There are no tenure, hours, or other eligibility requirements for employees.2
California’s Paid Sick Leave (PSL), established under the Healthy Workplaces, Healthy Families Act of 2014, entitles employees to take up to 40 hours or five days of leave for the diagnosis, care, or treatment of (or preventative care for) an employee or an employee’s family member. PSL applies to all employers, regardless of the number of employees. Employees are eligible to earn PSL after working for at least 30 days.3
The California Fair Employment and Housing Act (FEHA) entitles employees to five days of Bereavement Leave upon the death of a family member. A “family member” under this statute means a spouse, child, parent, sibling, grandparent, grandchild, domestic partner or parent-in-law. This applies to all employers with five or more employees. Employees are eligible to take bereavement leave after working for the same employer for at least 30 days.4
Employers have a right to demand loyalty from their employees while they are employed. This means that, during the term of employment, employers may legally prohibit an employee from competing or taking steps that would be detrimental to an employer’s ability to conduct business. However, contractual provisions applying those restrictions to a former employee—known as “covenants not to compete” or “non-competes”—are generally not allowed in California. California’s prohibition against non-competes has been around for many years and has made it difficult for California medical groups to prevent a former employee from competing directly, including joining a competing medical group. Effective January 1, 2024, the boundaries around what an employer may legally demand in this area have become even more limited, and the consequences for violators are significantly more severe.
First, a brief overview of the law before this year’s changes: California has long prohibited the enforcement of covenants not to compete with very narrow exceptions. (See Bus. & Prof. Code § 16600.) This contrasts with many other states where it is lawful for an employer to impose covenants not to compete so long as the duration and geographic area of the restriction are “reasonable.”
The one exception to California’s broad prohibition against the enforcement of non-competes is when a former employee was also an owner of the affiliated business. This area is legally complex, but generally, if the former employee was also an owner, then it’s possible for agreements to prohibit that employee from competing post-employment; however, such provisions must be carefully crafted, otherwise, a medical group employer can easily find itself unable to enforce such a provision.
With this background, in the last legislative session, two new bills were enacted into law: Assembly Bill No. 1076 and Senate Bill No. 699, both dealing with this subject. (Codified inBus. & Prof. Code §§ 16600.1, 16600.5, respectively.) Next, we will briefly review these two new laws.
AB 1076 reaffirms that covenants not to compete, unless they fall within a statutory exception, are void and unenforceable—but it goes beyond that. For the first time, it is now unlawful for employers to place unenforceable covenants not to compete in employment contracts, and, if the employer has any employment contracts that contain such covenants for employees who were employed after January 1, 2022, it must notify all such employees (and former employees) on or before February 14, 2024, that the provision is void. Failure to provide notice will constitute an act of “unfair competition” under California’s Unfair Competition Law (“UCL”) and subject the employer to the possibility of litigation and damages under that section. This makes it important that all employers have their employment contracts reviewed to assure that they do not contain any unlawful non-competes, and if they do, ensure such notifications are sent.
SB 699 adds additional teeth to the enforcement of non-compete violations, providing that any violation gives an employee the right to bring a private legal action, seeking an injunction, damages, and if such action is successful, reimbursement of attorneys’ fees by the employer. This means that, a former, or even current, employee can sue an employer for the mere presence of a non-compete provision, and not only obtain an injunction, but recover provable damages plus the cost of the employee’s attorneys’ fees in bringing such legal action.
SB 699 additionally clarifies that California laws against covenants not to compete prevail over contradictory laws that might otherwise apply in other states. Thus, if the employment is to be performed within California, California’s prohibitions against covenants not to compete will control (even, for example, if the employee lives outside of California).
If you would like advice on your employment contracts, please reach out to one of the listed attorneys.